Glucose transporter 2 (GLUT2) also known as solute carrier family 2 (facilitated glucose transporter), member 2 (SLC2A2) is a transmembrane carrier protein that enables protein facilitated glucose movement across cell membranes. It is the principal transporter for transfer of glucose between liver and blood[1] Unlike GLUT4, it does not rely on insulin for facilitated diffusion.
In humans, this protein is encoded by the SLC2A2gene.[2][3]
GLUT2 has high capacity for glucose but low affinity (high KM, ca. 15–20 mM) and thus functions as part of the "glucose sensor" in the pancreatic β-cells of rodents, though in human β-cells the role of GLUT2 seems to be a minor one.[8] It is a very efficient carrier for glucose.[9][10] Similarly, a recent study showed that lack of GLUT2 in β-cells doesn't impair glucose homeostasis or glucose-stimulated insulin secretion in mice.[11]
When the glucose concentration in the lumen of the small intestine goes above 30 mM, such as occurs in the fed-state, GLUT2 is up-regulated at the brush border membrane, enhancing the capacity of glucose transport. Basolateral GLUT2 in enterocytes also aids in the transport of fructose into the bloodstream through glucose-dependent cotransport.
Recent studies show that renal GLUT2 contributes to systemic glucose homeostasis by regulating glucose reabsorption.[7] Lack of renal Glut2 reversed features of diabetes and obesity in mice. In addition, renal Glut2 deficiency caused knockdown of renal Sglt2 through the transcription factor Hnf1α.[7]
Clinical significance
Defects in the SLC2A2 gene are associated with a particular type of glycogen storage disease called Fanconi-Bickel syndrome.[13]
In drug-treated diabetic pregnancies in which glucose levels in the woman are uncontrolled, neural tube and cardiac defects in the early-developing brain, spine, and heart depend upon functional GLUT2 carriers, and defects in the GLUT2 gene have been shown to be protective against such defects in rats.[14] However, whilst a lack of GLUT2 adaptability[15] is negative, it is important to remember the fact that the main result of untreated gestational diabetes appears to cause babies to be of above-average size, which may well be an advantage that is managed very well with a healthy GLUT2 status.
Maintaining a regulated osmotic balance of sugar concentration between the blood circulation and the interstitial spaces is critical in some cases of edema including cerebral edema.
GLUT2 appears to be particularly important to osmoregulation, and preventing edema-induced stroke, transient ischemic attack or coma, especially when blood glucose concentration is above average.[16] GLUT2 could reasonably be referred to as the "diabetic glucose transporter" or a "stress hyperglycemia glucose transporter."
SLC2A2 was associated with clinical stages and independently associated with overall survival in patients with Hepatocellular carcinoma, and could be considered a new prognostic factor for HCC.[17]
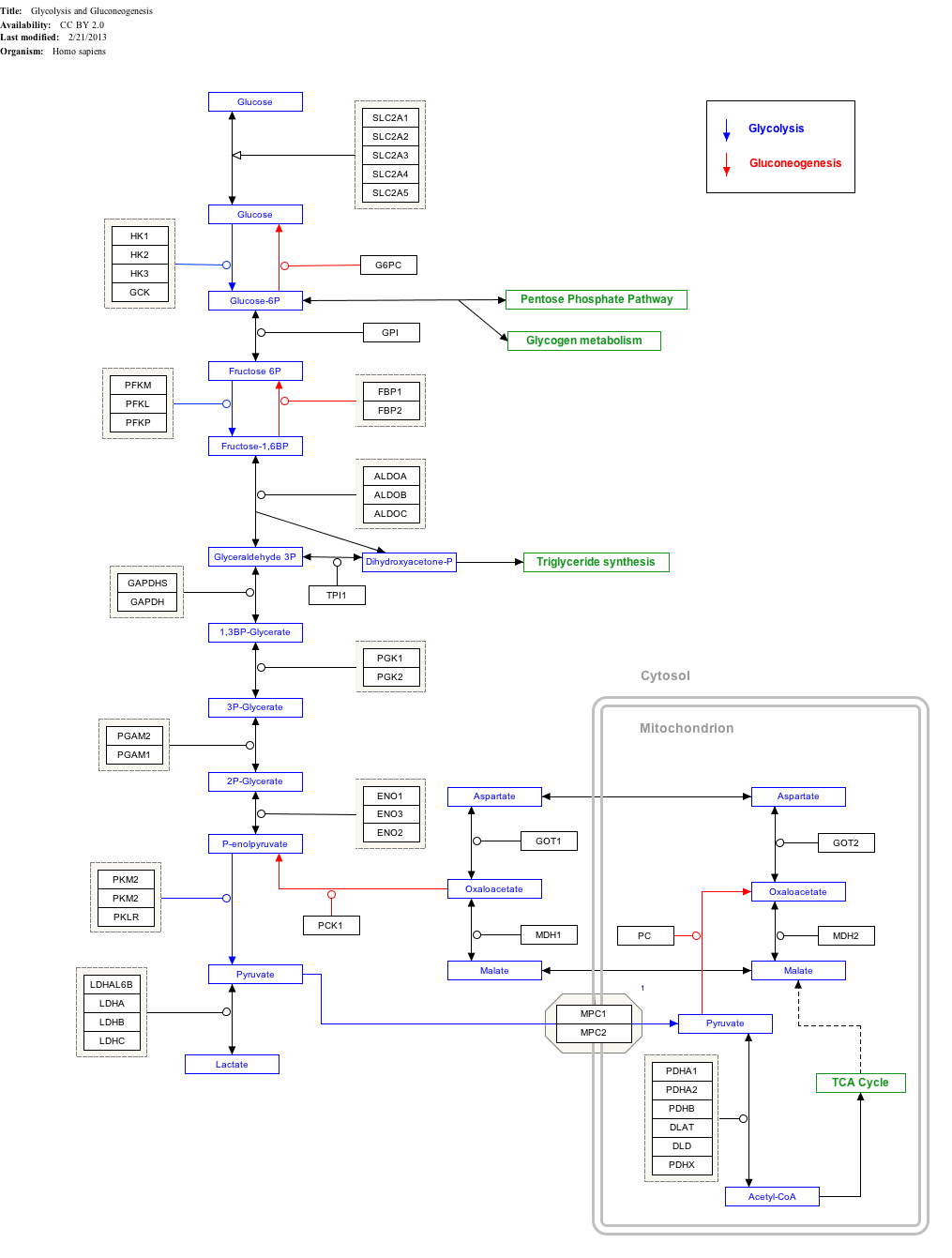
Interactive pathway map
Click on genes, proteins and metabolites below to link to respective articles.[§ 1]
^Gwyn W. Gould; Helen M. Thomas; Thomas J. Jess; Graeme I. Bell (May 1991). "Expression of human glucose transporters in Xenopus oocytes: kinetic characterization and substrate specificities of the erythrocyte, liver, and brain isoforms". Biochemistry. 30 (21): 5139–5145. doi:10.1021/bi00235a004. PMID2036379.
^McCulloch LJ, van de Bunt M, Braun M, Frayn KN, CLark A, Gloyn AL (December 2011). "GLUT2 (SLC2A2) is not the principal glucose transporter in human pancreatic beta cells: implications for understanding genetic association signals at this locus". Molecular Genetics and Metabolism. 104 (4): 648–53. doi:10.1016/j.ymgme.2011.08.026. PMID21920790.
^McCulloch LJ, van de Bunt M, Braun M, Frayn KN, Clark A, Gloyn AL (December 2011). "GLUT2 (SLC2A2) is not the principal glucose transporter in human pancreatic beta cells: implications for understanding genetic association signals at this locus". Molecular Genetics and Metabolism. 104 (4): 648–53. doi:10.1016/j.ymgme.2011.08.026. PMID21920790.
^Guillam MT, Hümmler E, Schaerer E, Yeh JI, Birnbaum MJ, Beermann F, Schmidt A, Dériaz N, Thorens B, Wu JY (November 1997). "Early diabetes and abnormal postnatal pancreatic islet development in mice lacking Glut-2". Nature Genetics. 17 (3): 327–30. doi:10.1038/ng1197-327. PMID9354799. S2CID37328600.
^Thomson AB, Wild G (March 1997). "Adaptation of intestinal nutrient transport in health and disease. Part I". Digestive Diseases and Sciences. 42 (3): 453–69. doi:10.1023/A:1018807120691. PMID9073126. S2CID25371741.

{kind=link}